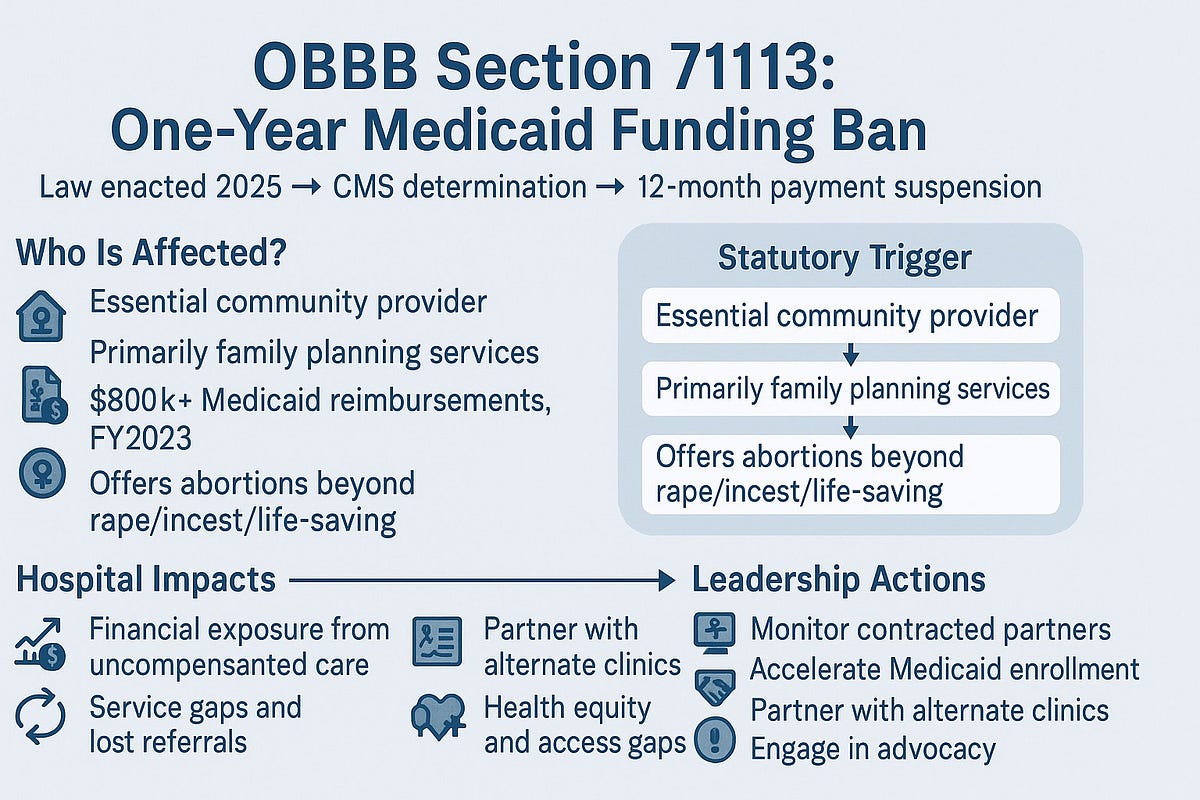

Section (71113) is a provision that withholds all federal Medicaid payments for twelve months from nonprofit “essential community providers” whose core business is reproductive and family planning care, if they both received at least $800,000 in combined federal and state Medicaid reimbursements during FY 2023 and deliver abortion services outside the limited exceptions of rape, incest, or life threatening emergencies. Although the language primarily addresses a narrow subset of safety net clinics, the downstream effects will impact hospitals that rely on these clinics for preventive and prenatal referrals, discharge planning, and continuity of care.
Section 71113 instructs the Centers for Medicare & Medicaid Services (CMS) to deny federal matching funds for any Medicaid claim submitted by a qualifying nonprofit provider for one year following the first day of the fiscal quarter in which CMS makes a non-compliance determination. The statute defines “qualifying nonprofit” through a three-part test: first, the entity must predominantly serve low-income or medically underserved patients; second, it must primarily furnish family planning and related reproductive services; third, it must have accepted over $800 in federal plus state Medicaid payments in FY 2023. CMS will recoup payments made in error and may impose additional civil monetary penalties. Notably, the ban applies to all Medicaid-covered services delivered by the provider, not just abortion care, replicating a mechanism that lawmakers have previously attempted to use against organizations such as Planned Parenthood , Cardinal & Pine, and the Center for Child and Family Policy.
Based on FY 2023 cost reports and Uniform Data System files, most entities meeting the statutory threshold are freestanding family planning clinics operating under Section 330 public health grants; roughly half hold Federally Qualified Health Center (FQHC) look-alike status. Planned Parenthood affiliates make up the largest block; yet, several regional Title X grantees, academic obstetrics departments with satellite reproductive health sites, and faith-based social service organizations also exceed the $800 mark. Nearly all of them qualify as “essential community providers” under the Affordable Care Act’s network adequacy rules, meaning state Medicaid agencies currently rely on their presence to meet access standards for contraception, sexually transmitted infection (STI) screening, and prenatal risk assessment. Removing federal match would force states to either substitute 100% state general funds for each affected claim, an improbable political choice, or to suspend the provider’s Medicaid contracts outright, creating service deserts in regions already marked by clinician shortages.
Although Section 71113 targets non-hospital entities, the financial shockwaves extend to acute care settings. A JAMA Viewpoint published last month estimates that for every one-dollar reduction in Medicaid spending on frontline reproductive health providers, hospitals absorb between $1.20 and $1.45 in additional uncompensated or charity care within eighteen months. Two factors drive the transfer: first, displaced patients lose their usual source of preventive care, leading to more costly emergencies; second, hospitals must maintain 24/7 on-call obstetric and gynecologic coverage without proportional reimbursement increases. Hospitals often serve as anchors in community health ecosystems. When reproductive health networks disintegrate, the public looks to us to fill the gap. Historical experience following Texas’s 2013 family planning cuts illustrates the risk: local hospitals saw sharp increases in non-Medicaid uncompensated obstetric care costs, and community trust eroded when patients perceived longer wait times and fewer options.
So, what can hospital leaders do to plan for these changes? First, map service line dependencies. Identify departments, such as obstetrics, neonatal intensive care, and infectious disease, that regularly receive referrals from essential community providers. Second, model budget scenarios under varying levels of clinic attrition. Use internal cost accounting to project the incremental expense of prenatal, labor, and delivery, and gynecologic emergency care delivered to uninsured patients. Third, strengthen on-site Medicaid enrollment programs to shorten application lags, thereby limiting the volume of unfunded episodes. Fourth, cultivate partnerships with alternative safety-net clinics, county health departments, and telehealth platforms that are capable of providing contraception counseling and STI testing. Finally, engage in state-level policy discussions. Several states are exploring stopgap grants or maintenance of effort provisions to backfill lost Medicaid match; timely advocacy can shape those mitigations.