Nearly 6 in 10 Americans (58 percent) say that Medicaid is either “very” or “somewhat” important to them and their family, according to the latest survey by the Kaiser Family Foundation. Those who say Medicaid is important to them believe that the America Health Care Act (AHCA), which passed the House of Representatives by a narrow 217–213 margin, would negatively impact their health care quality, access, and affordability.
They should be very worried. According to the Congressional Budget Office (CBO), the AHCA (aka, “Trumpcare”) would slash Medicaid funding by $834 billion by 2026 and drop 14 million people — children, the elderly, people with disabilities, or low-income adults — from coverage.
Furthermore, by a 71–26 percent margin, Americans overwhelmingly oppose the Trumpcare proposal to convert Medicaid into a block grant.

Under current law, the federal government and states share in the responsibility and costs of Medicaid. When there is population growth, an economic recession, a natural disaster, an epidemic, or needed investments to improve quality and access to care, the federal government and states share in the fiscal responsibility, as they do when there are cost savings.
Medicaid operates more efficiently than both Medicare or private health coverage. According to the Kaiser Family Foundation, “. . .if a typical low-income Medicaid adult or child were instead covered by private health insurance, total spending would be 26 percent higher for adults and 37 percent higher for children.”
Ironically, while Sally Pipes with the conservative Pacific Research Institute argues in favor of the AHCA’s $834 billion in Medicaid cuts, she simultaneously complains that Medicaid pays physicians less than Medicare and private insurers. To make her point, Pipes contents that “nearly one-third of doctors weren’t taking new Medicaid patients.”
First, even Pipes must see the irony is arguing for greater Medicaid spending on providers but supporting a policy that slashes the program by $834 billion with arbitrary funding caps that would preclude states from increasing provider payment rates. It simply makes no sense.
Second, Medicaid provider participation rates are no different than those in various private sector plans. Just like private health plans, Medicaid coverage is largely delivered through HMOs, which restrict access to providers in their network. Anyone that has an employer plan knows this challenge, as a simple medical procedure necessitates finding out whether an array of health professionals and institutions that may or may not be in your health plan. This is not at all unique to Medicaid.
Third, most states do respond to access concerns by either raising provider rates (which may not be allowable under a Medicaid per capita cap or block grant under the ACHA), easing provider enrollment restrictions, or targeting contracts to health providers and plans with stronger presence in medically underserved areas, to ensure that access to care measures for Medicaid remain strong. Data from Kaiser Family Foundation shows that has been working.

Cutting Medicaid by $834 billion would not solve anything. Instead, such cuts would do immense harm to the health coverage of vulnerable children.

Ironically, while Pipes argues Medicaid underpays providers, she also argues Medicaid is too expensive. But she is not alone. Other Medicaid critics include former Rep. David McIntosh with Club for Growth and Michael Needham with Heritage Action for America. They argue that Medicaid should be cut even further than the AHCA’s $834 billion in cuts.
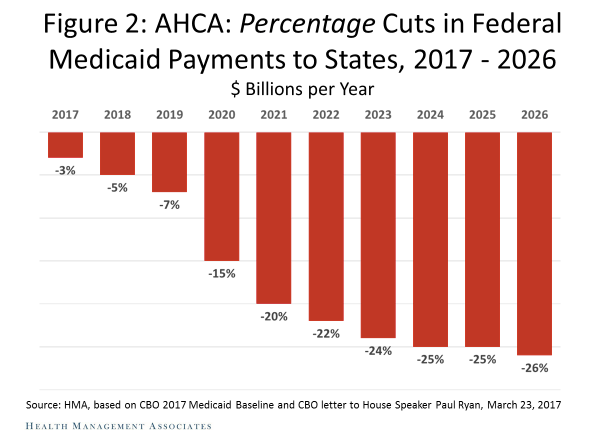
As this Health Management Associates (HMA) chart shows, states would have to dramatically increase spending in order to make up for these cuts — much less the provider payment increases that critics simultaneously urge. Since states across the country continue to face intense budget pressure, that is unlikely. So, what are states likely to do?

The Congressional Budget Office (CBO) gives us a good idea. As CBO explains:
. . .enrollees could face more significant effects if a state reduced providers’ payment rates or payments to managed care plans, cut covered services, or curtailed eligibility — either in keeping with current law or to a greater extent, if given the flexibility. If states reduced payment rates, fewer providers might be willing to accept Medicaid patients, especially given that, in many cases, Medicaid’s rates are already significantly below those of Medicare or private insurance for some of the same services. If states reduced payments to Medicaid managed care plans, some plans might shrink their provider networks, curtail quality assurance, or drop out of the program altogether. If states reduced covered services, some enrollees might decide either to pay out of pocket or to forgo those services entirely. And if states narrowed their categories of eligibility (including the optional expansion under the ACA), some of those enrollees would lose access to Medicaid coverage. . . .
Let’s be clear, none of this is good for children, people with disabilities, or senior citizens.
No reasonable person could argue that it would be good, which is why the American people strongly oppose the AHCA. In fact, according to a recent Quinnipiac University national poll, just 1 in 5 Americans, or 21 percent, support the AHCA. Moreover, the American people are over five times more likely to strongly disapprove of the AHCA rather than strongly approve of it.
Consequently, the Senate should listen to the American people, adopt the Hippocratic Oath and vow to “do no harm,” and firmly reject the AHCA.
And, let’s be honest. This bill isn’t really about cutting Medicaid in order to “improve” it. That is nonsensical. It is about providing a $664 billion tax cut to the wealthiest among us.

Now is the time to call your U.S. senators at 202–224–3121 and tell them to vote against the AHCA. The health and well-being of millions of Americans are at stake.