
Coronary artery disease is characterized by heart problems that result from atherosclerosis.[34] Atherosclerosis is a type of arteriosclerosis which is the “chronic inflammation of the arteries which causes them to harden and accumulate cholesterol plaques (atheromatous plaques) on the artery walls”.[35] CAD has several well-determined risk factors contributing to atherosclerosis. These risk factors for CAD include “smoking, diabetes, high blood pressure (hypertension), abnormal (high) amounts of cholesterol and other fat in the blood (dyslipidemia), type 2 diabetes and being overweight or obese (having excess body fat)” due to lack of exercise and a poor diet.[36] Some other risk factors include high blood pressure, smoking, diabetes, lack of exercise, obesity, high blood cholesterol, poor diet, depression, family history, psychological stress and excessive alcohol.[6][7][18] About half of cases are linked to genetics.[37] Apart from these classical risk factors, several unconventional risk factors have also been studied including high serum fibrinogen, high c-reactive protein (CRP), chronic inflammatory conditions, hypovitaminosis D, high lipoprotein A levels, serum homocysteine etc.[38][39] Smoking and obesity are associated with about 36% and 20% of cases, respectively.[40] Smoking just one cigarette per day about doubles the risk of CAD.[41] Lack of exercise has been linked to 7–12% of cases.[40][42] Exposure to the herbicide Agent Orange may increase risk.[43] Rheumatologic diseases such as rheumatoid arthritis, systemic lupus erythematosus, psoriasis, and psoriatic arthritis are independent risk factors as well.[44][45][46][47][excessive citations]
Job stress appears to play a minor role, accounting for about 3% of cases.[40] In one study, females who were free of stress from work life saw an increase in the diameter of their blood vessels, leading to decreased progression of atherosclerosis.[48] In contrast, females who had high levels of work-related stress experienced a decrease in the diameter of their blood vessels and significantly increased disease progression.[48]
Air pollution
Air pollution, both indoor and outdoor, is responsible for roughly 28% of deaths from CAD. This varies by region: In highly developed areas, this is approximately 10%, whereas in Southern, East and West Africa, and South Asia, approximately 40% of deaths from CAD can be attributed to unhealthy air.[49] In particular, fine particle pollution (PM2.5), which comes mostly from the burning of fossil fuels, is a key risk factor for CAD.[50]
Blood fats
The consumption of different types of fats including trans fat (trans unsaturated), and saturated fat, in a diet “influences the level of cholesterol that is present in the bloodstream”.[51] Unsaturated fats originate from plant sources (such as oils). There are two types of unsaturated fats, cis and trans isomers. Cis unsaturated fats are bent in molecular structure and trans are linear. Saturated fats originate from animal sources (such as animal fats) and are also molecularly linear in structure.[52] The linear configurations of unsaturated trans and saturated fats allow them to easily accumulate and stack at the arterial walls when consumed in high amounts (and other positive measures towards physical health are not met).
- Fats and cholesterol are insoluble in blood and thus are amalgamated with proteins to form lipoproteins for transport. Low-density lipoproteins (LDL) transport cholesterol from the liver to the rest of the body and raise blood cholesterol levels. The consumption of “saturated fats increases LDL levels within the body, thus raising blood cholesterol levels”.[51]
- High-density lipoproteins (HDL) are considered ‘good’ lipoproteins as they search for excess cholesterol in the body and transport it back to the liver for disposal. Trans fats also “increase LDL levels whilst decreasing HDL levels within the body, significantly raising blood cholesterol levels”.[51]
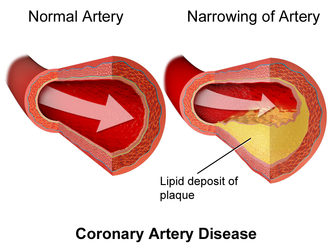
High levels of cholesterol in the bloodstream lead to atherosclerosis. With increased levels of LDL in the bloodstream, “LDL particles will form deposits and accumulate within the arterial walls, which will lead to the development of plaques, restricting blood flow”.[51] The resultant reduction in the heart’s blood supply due to atherosclerosis in coronary arteries “causes shortness of breath, angina pectoris (chest pains that are usually relieved by rest), and potentially fatal heart attacks (myocardial infarctions)”.[36]
Genetics
The heritability of coronary artery disease has been estimated between 40% and 60%.[53] Genome-wide association studies have identified over 160 genetic susceptibility loci for coronary artery disease.[54]
Transcriptome
Several RNA Transcripts associated with CAD – FoxP1, ICOSLG, IKZF4/Eos, SMYD3, TRIM28, and TCF3/E2A are likely markers of regulatory T cells (Tregs), consistent with known reductions in Tregs in CAD.[55]

The RNA changes are mostly related to ciliary and endocytic transcripts, which in the circulating immune system would be related to the immune synapse.[56] One of the most differentially expressed genes, fibromodulin (FMOD), which is increased 2.8-fold in CAD, is found mainly in connective tissue[57] and is a modulator of the TGF-beta signaling pathway. However, not all RNA changes may be related to the immune synapse. For example, Nebulette, the most down-regulated transcript (2.4-fold), is found in cardiac muscle; it is a ‘cytolinker’ that connects actin and desmin to facilitate cytoskeletal function and vesicular movement. The endocytic pathway is further modulated by changes in tubulin, a key microtubule protein, and fidgetin, a tubulin-severing enzyme that is a marker for cardiovascular risk identified by genome-wide association study. Protein recycling would be modulated by changes in the proteasomal regulator SIAH3 and the ubiquitin ligase MARCHF10. On the ciliary aspect of the immune synapse, several of the modulated transcripts are related to ciliary length and function. Stereocilin is a partner to mesothelin, a related super-helical protein, whose transcript is also modulated in CAD. DCDC2, a double-cortin protein, modulates ciliary length. In the signaling pathways of the immune synapse, numerous transcripts are directly related to T-cell function and the control of differentiation. Butyrophilin is a co-regulator for T cell activation. Fibromodulin modulates the TGF-beta signaling pathway, a primary determinant of Tre differentiation. Further impact on the TGF-beta pathway is reflected in concurrent changes in the BMP receptor 1B RNA (BMPR1B), because the bone morphogenic proteins are members of the TGF-beta superfamily, and likewise impact Treg differentiation. Several of the transcripts (TMEM98, NRCAM, SFRP5, SHISA2) are elements of the Wnt signaling pathway, which is a major determinant of Treg differentiation.
Other
- Endometriosis in females under the age of 40.[58]
- Depression and hostility appear to be risks.[59]
- The number of categories of adverse childhood experiences (psychological, physical, or sexual abuse; violence against mother; or living with household members who used substances, mentally ill, suicidal, or incarcerated) showed a graded correlation with the presence of adult diseases including coronary artery (ischemic heart) disease.[60]
- Hemostatic factors: High levels of fibrinogen and coagulation factor VII are associated with an increased risk of CAD.[61]
- Low hemoglobin.[62]
- In the Asian population, the b fibrinogen gene G-455A polymorphism was associated with the risk of CAD.[63]
- Patient-specific vessel ageing or remodelling determines endothelial cell behaviour and thus disease growth and progression. Such ‘hemodynamic markers’ are patient-specific risk surrogates.[64]
- HIV is a known risk factor for developing atherosclerosis and coronary artery disease.[65]