Poisoning and drug overdoses remain major global health challenges, leading to countless emergency department visits and fatalities each year. Antidotes play a life-saving role by neutralizing toxins, reversing drug overdoses, or counteracting harmful effects of medications.
Antidotes are essential tools in emergency and toxicology medicine, providing rapid, targeted reversal of life-threatening drug overdoses and poisonings. Knowledge of these agents—their suffixes, mechanisms, and clinical applications—empowers clinicians to make timely, life-saving interventions.
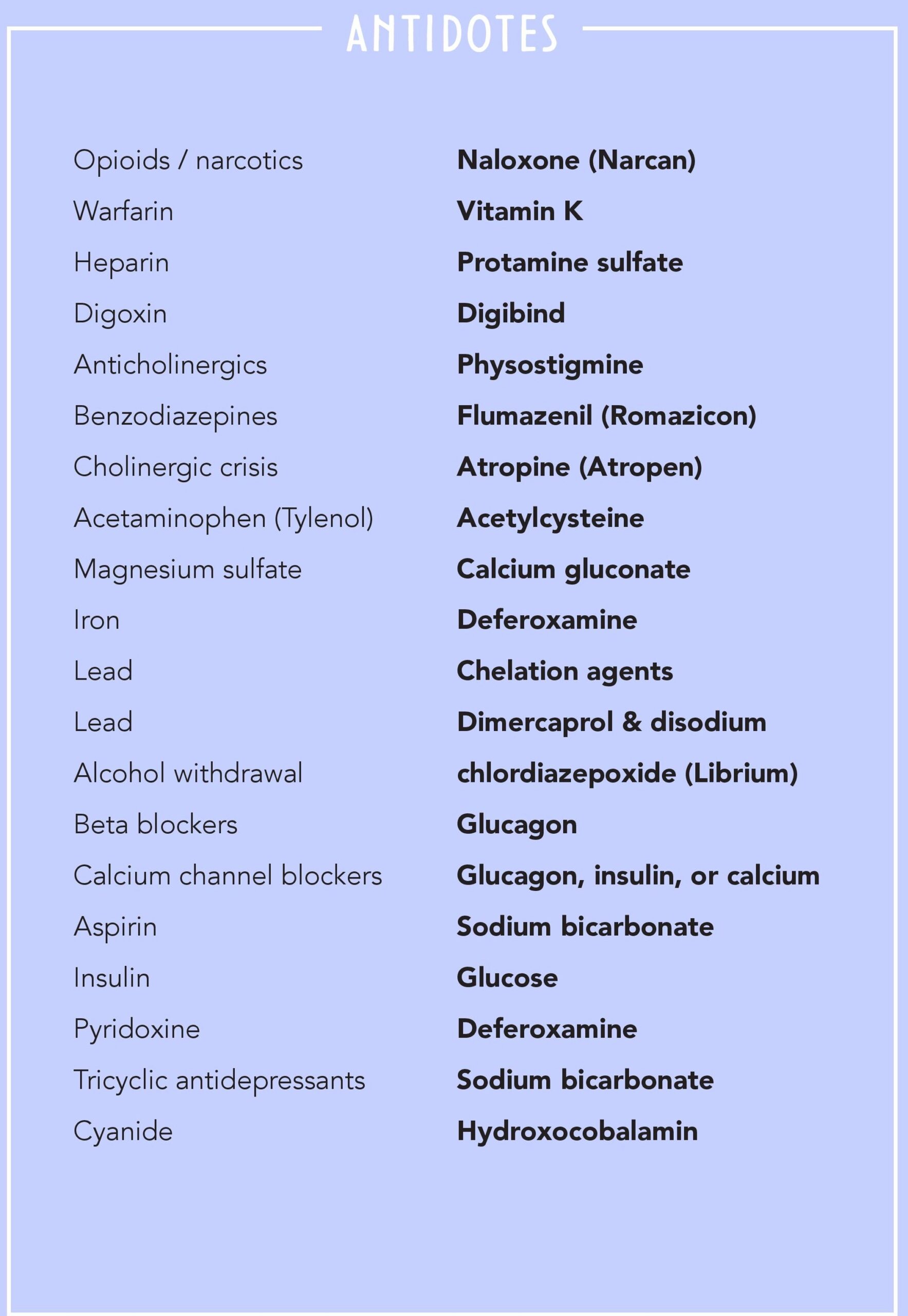
Major Antidotes and Their Applications

1. Opioid/Narcotic Overdose
Antidote: Naloxone (Narcan)
Mechanism: Competitive antagonist at μ-opioid receptors → rapidly reverses respiratory depression.
Uses: Overdose from heroin, morphine, oxycodone, fentanyl.
Key Point: Short half-life → repeated dosing or infusion may be required.
2. Warfarin Toxicity
Antidote: Vitamin K
Mechanism: Restores synthesis of vitamin K–dependent clotting factors (II, VII, IX, X).
Uses: Reverses warfarin-induced bleeding.
Alternative: Fresh frozen plasma (FFP) or prothrombin complex concentrate (PCC) for severe cases.
3. Heparin Toxicity
Antidote: Protamine sulfate
Mechanism: Positively charged protamine binds negatively charged heparin → neutralization.
Uses: Heparin overdose, reversal during cardiac surgery.
4. Digoxin Toxicity
Antidote: Digibind (Digoxin-specific antibody fragments)
Mechanism: Binds digoxin → prevents binding to Na+/K+ ATPase → reversal of arrhythmias and toxicity.
Uses: Severe digoxin overdose (arrhythmias, hyperkalemia).
5. Anticholinergic Toxicity
Antidote: Physostigmine
Mechanism: Reversible acetylcholinesterase inhibitor → increases acetylcholine levels → reverses delirium, tachycardia, hyperthermia.
Uses: Overdose of atropine, antihistamines, tricyclic antidepressants (with caution).
6. Benzodiazepine Overdose
Antidote: Flumazenil (Romazicon)
Mechanism: GABA-A receptor antagonist → reverses sedation and respiratory depression.
Uses: Diazepam, alprazolam, lorazepam overdose.
Caution: May trigger seizures in chronic benzodiazepine users.
7. Cholinergic Crisis (e.g., organophosphate poisoning)
Antidote: Atropine (Atropen)
Mechanism: Blocks muscarinic receptors → reduces secretions, bronchospasm, bradycardia.
Often Combined With: Pralidoxime (2-PAM) to regenerate acetylcholinesterase.
8. Acetaminophen (Paracetamol/Tylenol) Overdose
Antidote: Acetylcysteine (NAC)
Mechanism: Restores glutathione → detoxifies harmful metabolite (NAPQI).
Uses: Prevents liver damage if given within 8–10 hours of overdose.
9. Magnesium Sulfate Toxicity
Antidote: Calcium gluconate
Mechanism: Antagonizes magnesium’s effect at neuromuscular junction.
Uses: Overdose during eclampsia treatment.
10. Iron Poisoning
Antidote: Deferoxamine
Mechanism: Chelates free iron → excreted in urine.
Uses: Acute iron toxicity (common in children after accidental ingestion).
11. Lead Poisoning
Antidotes: Chelation agents such as EDTA, dimercaprol, succimer.
Mechanism: Bind lead → excretion via urine.
Uses: Chronic or acute lead toxicity (children and workers at risk).
12. Alcohol Withdrawal
Antidote/Management Drug: Chlordiazepoxide (Librium)
Mechanism: Long-acting benzodiazepine → prevents seizures, delirium tremens.
Uses: Alcohol detoxification programs.
13. Beta-Blocker Overdose
Antidote: Glucagon
Mechanism: Activates adenylate cyclase via glucagon receptors → ↑ cAMP → improved heart rate and contractility.
Uses: Severe hypotension, bradycardia from propranolol or metoprolol overdose.
14. Calcium Channel Blocker Overdose
Antidotes: Glucagon, insulin with glucose, or calcium infusion
Mechanism: Improve cardiac contractility and conduction.
Uses: Verapamil, diltiazem, amlodipine overdose.
15. Aspirin (Salicylate) Poisoning
Antidote: Sodium bicarbonate
Mechanism: Alkalinizes urine → enhances salicylate excretion.
Uses: Severe aspirin toxicity with metabolic acidosis.
16. Insulin Overdose
Antidote: Glucose (IV or oral)
Mechanism: Restores blood sugar levels.
Uses: Severe hypoglycemia in diabetic patients.
17. Pyridoxine (Isoniazid Toxicity)
Antidote: Deferoxamine (iron chelator used here in special cases) OR Vitamin B6 supplementation
Mechanism: Replenishes pyridoxine deficiency caused by isoniazid.
Uses: Prevention/treatment of seizures in isoniazid toxicity.
18. Tricyclic Antidepressant (TCA) Toxicity
Antidote: Sodium bicarbonate
Mechanism: Stabilizes cardiac membranes, prevents arrhythmias.
Uses: Overdose from amitriptyline, nortriptyline.
19. Cyanide Poisoning
Antidote: Hydroxocobalamin
Mechanism: Binds cyanide to form cyanocobalamin (Vitamin B12), excreted in urine.
Uses: Cyanide exposure from fires, lab accidents, industrial poisoning.
Quick Reference Table
| Poison/Toxicity | Antidote | Mechanism | Clinical Notes |
|---|---|---|---|
| Opioids | Naloxone | μ-receptor antagonist | Life-saving in opioid overdose |
| Warfarin | Vitamin K | Restores clotting factors | Use with PCC/FFP in emergencies |
| Heparin | Protamine sulfate | Neutralizes heparin | Used in surgery reversal |
| Digoxin | Digibind | Binds digoxin | For arrhythmias, hyperkalemia |
| Benzodiazepines | Flumazenil | GABA-A antagonist | Risk of seizures |
| Acetaminophen | Acetylcysteine | Restores glutathione | Best within 10 hrs |
| Iron | Deferoxamine | Chelation therapy | Red urine color (vin rose urine) |
| Lead | EDTA, dimercaprol | Chelation therapy | Pediatric poisoning |
| Beta-blockers | Glucagon | ↑ cAMP, cardiac output | First-line antidote |
| Calcium channel blockers | Glucagon, calcium, insulin | Restores contractility | ICU support |
| Aspirin | Sodium bicarbonate | Urine alkalinization | Enhances excretion |
| Cyanide | Hydroxocobalamin | Converts to Vitamin B12 | Preferred safe antidote |
Frequently Asked Questions (FAQs)
Q1. Why is naloxone preferred over naltrexone in opioid overdose?
Naloxone works rapidly and is short-acting, making it suitable for emergency reversal, while naltrexone is long-acting and used in addiction therapy.
Q2. What is the difference between acetylcysteine and methionine in paracetamol poisoning?
Both replenish glutathione, but acetylcysteine (NAC) is the gold standard due to better efficacy.
Q3. Why is flumazenil rarely used in benzodiazepine overdose?
It can precipitate seizures in chronic benzodiazepine users or those with mixed drug overdoses (especially with TCAs).
Q4. Which antidote is used for both beta-blocker and calcium channel blocker overdose?
Glucagon is common to both, but calcium and high-dose insulin are specifically useful for calcium channel blocker toxicity.
Q5. How does sodium bicarbonate work in aspirin and TCA poisoning?
By alkalinizing urine, it enhances excretion (aspirin) and stabilizes cardiac membranes (TCA overdose).
Q6. Why is hydroxocobalamin safer than older cyanide antidotes?
Unlike nitrites, hydroxocobalamin does not induce methemoglobinemia and directly converts cyanide to excretable vitamin B12.