CENTRAL HYPOTHYROIDISM CAN TAKE CHILD, YOUTH-FAILURE HYPOTHALAMIC-PITUITARY-LOW HEIGHT.
IF THE TOTAL T4 TSH BE FREE AND LOW, THE POSSIBILITY OF CENTRAL HYPOTHYROIDISM (FAILURE HYPOTHALAMIC OR PITUITARY) SHOULD BE CONSIDERED (THIS WOULD NOT BE DETERMINED IN TESTS OF NEWBORN SCREENING WHICH USED PRIMARILY THE TRACKING TSH). THIS DYSFUNCTION IS INVARIABLY TOGETHER WITH AMENDMENTS OF GH AND OTHER DISORDERS THE CENTRAL NERVOUS SYSTEM, IN THESE SITUATIONS LINEAR LOW HEIGHT FIGURE IS A FREQUENT IN DISORDERS. PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO.
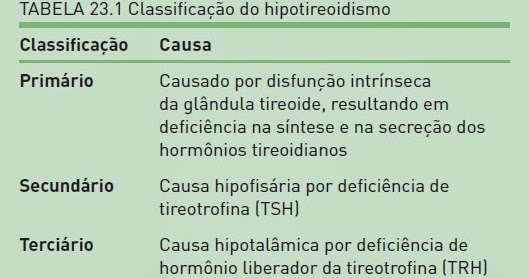
Hypothyroidism (underactive thyroid gland), is a common endocrine disorder in which the thyroid gland does not produce enough thyroid hormone. It can cause a range of symptoms, such as tiredness, inability to cold tolerate, and weight gain. In children, hypothyroidism leads to stunted growth and intellectual development and inducing longitudinal or linear low stature, and in case of delayed mental age compared with chronological age which is called cretinism in severe cases. The diagnosis of hypothyroidism, when suspected, can be confirmed with blood tests that measure thyroid stimulating hormone (TSH) and thyroxine (levels). However, central hypothyroidism has important peculiarities; Central hypothyroidism is defined as the hypothyroidism due to insufficient stimulation by thyroid stimulating hormone (TSH) in an otherwise normal thyroid gland. It has an estimated prevalence of about 1 at 80.000 to 1 in 120.000. May be secondary (pituitary) or tertiary hypothyroidism (hypothalamus) in origin, in other words is a disease originating on neuroendocrine disorders through the involvement of pituitary and hypothalamic arcuate nucleus that will compromise or secondary or tertiary endocrine producing effector substances called thyroid functions.
Dr. João Santos Caio Jr.
Endocrinologia – Neuroendocrinologista
CRM 20611
Dra. Henriqueta V. Caio
Endocrinologista – Medicina Interna
CRM 28930
Como saber mais:
1. Cerca de 1 em 3.500 crianças nos EUA são diagnosticadas com DGH (Lindsay et al. 1994). Apenas 20% destas crianças têm DGH orgânica…
http://hormoniocrescimentoadultos.blogspot.com
2. As causas orgânicas incluem tumores do sistema nervoso central, radiação, infecção e lesão cerebral traumática…
http://longevidadefutura.blogspot.com
3. Aproximadamente 80% das crianças não têm uma causa prontamente identificável de DGH…
http://imcobesidade.blogspot.com
AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO
DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA.
Referências Bibliográficas:
Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Ezzat S, Asa SL, Couldwell WT, et al: The prevalence of pituitary adenomas: A systematic review. Cancer 2004;101:613-619; Krikorian A, Aron D: Evaluation and management of pituitary incidentalomas—revisiting an acquaintance. Nat Clin Pract Endocrinol Metab 2006;2:138-145; Molitch ME, Clemmons DR, Malozowski S, et al: Evaluation and treatment of adult growth hormone deficiency: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2006;9:1621-1634; Casanueva FF, Molitch ME, Schlechte JA, et al: Guidelines of the pituitary society for the diagnosis and management of prolactinomas. Clinical Endocrinology 2006;65:265-273; Schade R, Andersohn F, Suissa S, et al: Dopamine agonists and the risk of cardiac-valve regurgitation. N Engl J Med 2007;356:29-38; Nachtigall LB, Valassi E, MCarty D, et al: Cardiac valvular function in hyperprolactinemic patients receiving cabergoline. Oral abstract 27-2, 90th Annual Endocrine Society Meeting, San Francisco, June 2008; Bonadonna S, Doga M, Gola M, et al: Diagnosis and treatment of acromegaly and its complications: Consensus guidelines. J Endocrinol Invest 2005;28(11 Suppl):43-47; Ezzat S, Serri O, Chik CL, et al: Canadian consensus guidelines for the diagnosis and management of acromegaly. Clin Invest Med 2006;29:29-39; Findling JW, Raff H: Cushing’s syndrome: Important issues in diagnosis and management. J Clin Endocrinol Metab 2006;91:3746-3753; Arnaldi G, Angeli A, Atkinson AB, et al: Diagnosis and complications of Cushing’s syndrome: A consensus statement. J Clin Endocrinol Metab 2003;88(12):5593-5602.