Around 2015, Gov. Greg Abbott reiterated his stance on refusing to expand Medicaid in Texas. This left more than 1 million Texans without health insurance who were “too poor to receive federal subsidies for private health insurance under the Affordable Care Act but too rich to qualify for coverage under Texas’ current Medicaid requirements” (Walters). Whether this would be beneficial or detrimental to Texans was constantly debated, and Medicaid expansion is still is a topic of discussion today. This report seeks to analyze how possession of Medicaid affected cancer patients in Texas in 2015.
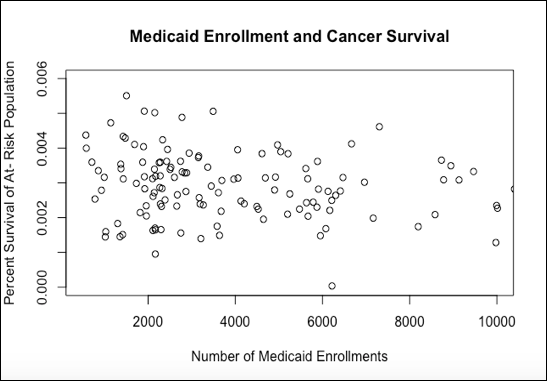
Table 1 displays that counties with higher Medicaid enrollments are not correlated with higher cancer survival rates. The following discussion will seek to determine why this could be the case.

Disparities exist in outcomes of people who are Medicaid- enrolled before diagnosis of cancer, Medicaid-enrolled after diagnosis, and people who are not enrolled in Medicaid at all. In a study of Michigan cancer patients, subjects who enrolled in Medicaid after cancer diagnoses had significantly lower survival rates across an 8-year span relative to non‐Medicaid subjects (Bradley 2005). The individuals who were not enrolled in Medicaid had better chances of survival than those who were enrolled in Medicaid after a late-stage diagnosis. This is consistent with Table 1, that the possession of Medicaid is not a predictor of survival. No correlation was found between incidence of cancer (per 100,000 people) and Medicaid enrollment (Table 1). Thus, the idea that possessing Medicaid increases chances of survival is false.
In a June 2017 study in the journal Cancer Epidemiology, researchers found that more patients were diagnosed with Stage 1 breast cancer after the Affordable Care Act took effect. Having insurance would increase a patient’s chance of getting a diagnosis because individuals who have insurance generally have regular doctors’ visits (Silva). A positive correlation in high-risk counties with Medicaid enrollment exists (Table 2). However, of the at-risk population, there is no increase in survival percentages of the at-risk population for Medicaid holders (Table 1). A confounding factor that may explain why no correlation exists between Medicaid enrollment and cancer survival for the 2015 data for Texas is that those with late-stage cancer obtained Medicaid after diagnosis. Bradley’s 2001 study explains that by the time Medicaid is obtained by an individual with late stage cancer, the individual has around the same chance of survival as someone without insurance.

One failure of my analysis is that it does not differentiate between cancer incidences and cancer related deaths from people who obtained Medicaid after diagnosis, and those who had Medicaid before diagnosis. Bradley’s multiple studies display better survival rates of those without Medicaid compared to those with Medicaid and a late-stage cancer diagnosis. This explains that the possession of Medicaid is not the only answer to increasing survival of cancer patients, and therefore Bradley’s studies provides an explanation for my own data analysis. It is the combination of Medicaid and an early diagnosis that increases survival of cancer patients. The positive correlation found in my analysis between counties with a high at-risk population for cancer and enrollments in Medicaid shows that patients are receiving insurance who have a higher risk of cancer, however this is not translating into higher percentage of survival rates (Table 1). This can be explained by late-stage diagnoses driving the survival rate down.
In a New Jersey study relating Medicaid holders and breast cancer patients, disparities were found in survival of those who possess Medicaid and those who are privately insured. Dr. Ayanian found that at the diagnosis of disease, women covered by Medicaid and uninsured women both have more advanced diseases than privately insured women. There was a positive relationship in advancement of breast cancer and possession of Medicaid: it is possible that women who possess Medicaid are more prone to having a late-stage diagnosis. This study also found that “survival during the 54 to 89 months after diagnosis was significantly worse for uninsured patients and those covered by Medicaid than for privately insured patients with local disease” (Ayanian).
Both the Bradley and Ayanian studies find that there is a comparable chance of survival for patients with late-stage cancer who have Medicaid versus patients who do not have Medicaid. Ayanian found that privately insured women have increased survival rates, which could be because privately insured women are more likely to be white, married, and not living in poor communities. Additionally, both Medicaid holders and non-insured women in the Ayanian study “had more coexisting diagnoses than privately insured women”. The adjusted risk of death was 40 percent higher or Medicaid patients than for privately insured patients. Poorer people and those of color are more likely to have Medicaid, which could act as confounding factors as to why those with Medicaid are more likely to have coexisting diagnoses (Ayanian).
A 2006 nation-wide study also found that “who are uninsured or are insured by Medicaid are more likely to present with more advanced cancer” (Kwok). Kwok’s study supplements the data found in the isolated New Jersey and Michigan studies, and furthers the case that possession of Medicaid alone will not necessarily increases the chances of a patient’s survival, consistent with Table 1. Bradley’s study explained that early diagnosis is key to survival, but if Kwok and Ayanian’s studies both found that citizens with Medicaid tend to have later stage cancer to begin with, then just having Medicaid may not be helpful in actually detecting cancer earlier. However, more analysis must be conducted before a concrete conclusion can be drawn.
Therefore, in order to create healthcare policy that truly increases cancer survival, more than just Medicaid possession must be taken into account. An emphasis on detecting cancer early for those with and without Medicaid could be the missing link in increasing cancer survival rates not only in Texas but throughout the country, especially for minorities and those living in low income areas.
Sources
Data accessed from
Texas Comptroller Database: Cancer Incidence File
Texas Comptroller Database: Cancer Mortality File
Texas Health and Human Services: Historical Medicaid Enrollment 2015
All charts were created using ‘R’ from data accessed from the sources above.