The Centers for Medicare and Medicaid Services (CMS) recently issued a draft rule that could dramatically improve access to innovative evidence-based treatment that would be delivered virtually. In particular, the Medicare Coverage for Innovative Technology (MCIT) initiative proposes a new Medicare coverage pathway for Food and Drug Administration (FDA) designated breakthrough medical devices. The Breakthrough Devices Program (BDP) was created in response to the 21st Century Cures Act (Cures Act), enacted in December 2016. The BDP is a voluntary program for certain medical devices that provide for more effective treatment or diagnosis of life-threatening or irreversibly debilitating diseases or conditions. The MCIT proposal would provide four years of provisional national Medicare coverage on the same day as FDA market authorization for breakthrough devices. While this new coverage pathway would offer beneficiaries nation-wide predictable access to new, breakthrough devices to help improve their health outcomes, a major limitation of the proposed rule is that if an FDA-cleared technology does not have a benefit category, then it will not get coverage in the Medicare program under the MCIT initiative.
Unfortunately, under the Medicare program’s current but outdated interpretation of regulatory language, digital therapeutics, one of the most common types of breakthrough-designated technologies, do not have a benefit category recognized by CMS. Digital therapeutics, a subset of digital health, are evidence-based therapeutic interventions driven by high quality software programs to prevent, manage, or treat a medical disorder or disease. Digital therapeutics are most commonly regulated under the Software-as-a-Medical-Device (SaMD) framework, though not everything with SaMD is a digital therapeutic. Similar to digital therapeutics, digital diagnostics can be treated as SaMD and the arguments herein are applicable to both digital therapeutics and digital diagnostics. SaMD is defined by the FDA and the International Medical Device Regulators Forum (IMDRF) as software intended to be used for one or more medical purposes that perform these purposes without being part of a hardware medical device. Digital therapeutics have enormous potential to improve health outcomes for Medicare beneficiaries, especially during and beyond the COVID19 pandemic. But their opportunity for impact is dramatically limited by the lack of a Medicare benefit category for digital therapeutics as SaMD according to CMS’s interpretation to date.
Medicare reimbursement for digital therapeutics could happen through congressional or regulatory action. Congress could establish a Medicare benefit category for digital therapeutics similar to the way they established a category for mammography screening through the Medicare Catastrophic Coverage Act of 1988, preventive benefits through the Patient Protection and Affordable Care Act (ACA) in 2010, home infusion therapy through the 21st Century Cures Act in 2016, and opioid use disorder treatment services through the SUPPORT Act in 2018. There is currently a bill called the Access to Prescription Digital Therapeutics Act of 2020 with bipartisan support in the Senate, however the Congressional stalemate makes that bill’s advancement unlikely during this Congress.
While a legislative solution would be welcome, the MCIT has introduced a more timely mechanism to ensure patients get access to evidence-based treatment safely in their homes. In light of the maturation of the digital therapeutics space and the COVID19 public health crisis, CMS could use the MCIT rule to clearly state that the existing benefit category, durable medical equipment (DME), applies to many digital therapeutics and clarify that breakthrough-designated SaMD could be subject to this coverage and subsequent payment.
Current FDA and CMS Process
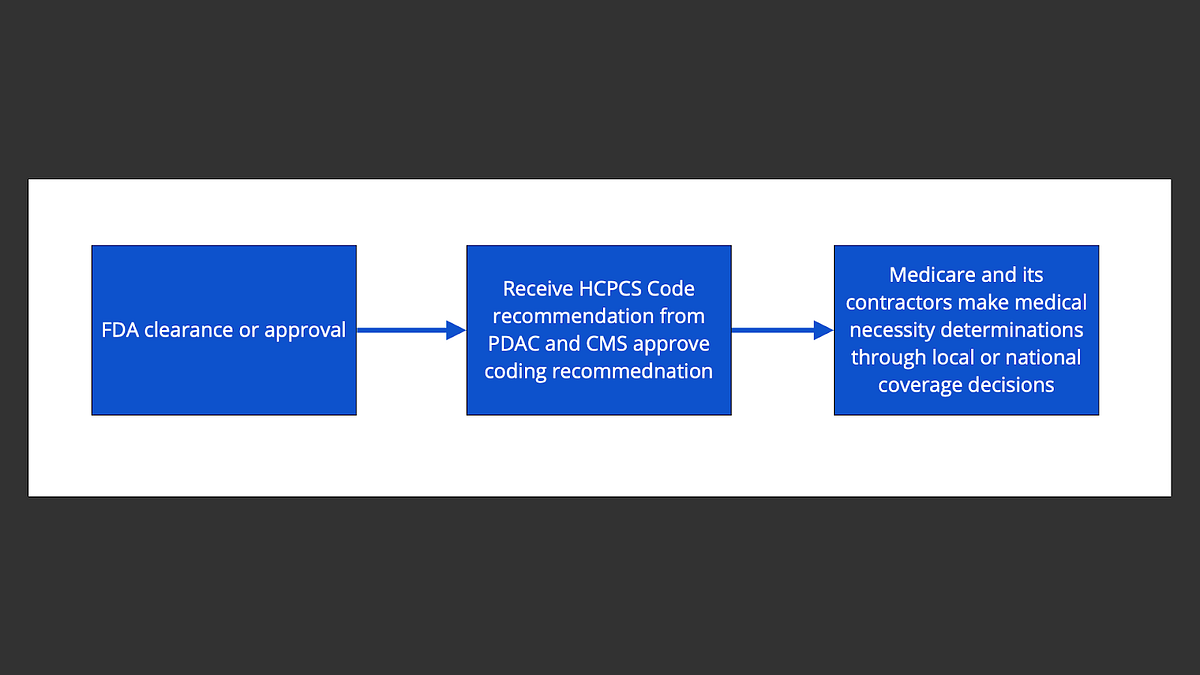
In order for a Medicare benefit to receive coverage and be reimbursable, it must first have a code to describe the benefit. (Figure 1) The code development process varies depending on the type of Medicare benefit that is being proposed. Since many breakthrough-designated SaMD technologies can be viewed as DME as the authors explain later, the current pathway of FDA approval and Medicare coding and coverage will be reviewed for devices that qualify as a DME benefit.
Figure 1: Current FDA Approval and Medicare Coding and Coverage Processes for DME
The first step in the process is applying for breakthrough designation. The next step is securing FDA clearance or approval. Most SaMD technologies seeking FDA clearance will pursue the 510k application, also known as the pre-market notification (PMN) route, or a de novo 510k application. (Figure 2) Other SaMD technologies seeking FDA approval rather than clearance may submit a Pre-Market Approval (PMA) application. If they meet class II (moderate risk) requirements, the devices are cleared by the FDA to be marketed based on substantial equivalence to existing predicate devices. If they meet class III (high risk) requirements, the devices must be approved by the FDA to be marketed.
Figure 2: FDA clearance and approval process
Once a device is FDA cleared or approved, it then must obtain a DME code assigned through the Medicare Contractor for Pricing, Data Analysis and Coding HCPCS Level II DMEPOS Codes (PDAC). The PDAC follows the CMS Healthcare Common Procedure Coding System (HCPCS) decision tree for external requests to add or revise a HCPCS code. (Figure 3)
In addition to this HCPCS decision tree, devices also have to meet the regulatory definition of DME according to 42 C.F.R. § 414.202 which includes a five-prong test. To be considered DME by CMS, the equipment must:
- Withstand repeated use
- Have an expected life of 3 years
- Be primarily and customarily used to serve a medical purpose
- Generally not be useful in the absence of an illness or injury
- Be appropriate for use in the home
Once PDAC comes to a coding recommendation, it then sends its recommendation to the HCPCS working group at CMS. If the CMS HCPCS working group agrees with the PDAC recommendation, the device is then given a new code or a miscellaneous code and is deemed to be DME.
Figure 3: HCPCS Decision Tree
Once there is a code, Medicare then makes a coverage decision if and how much a code will be reimbursed. Medicare can only cover an item or service if (1) there is an available benefit category; (2) the item or service is medically necessary; and (3) no other provision of the Medicare statute operates to exclude the item or service from coverage (e.g., dental services, eyeglasses, hearing aids). Typically, Medicare and its contractors make medical necessity determinations through local or national coverage determinations (NCDs). In the absence of a coverage decision, an item or service is covered on a case-by-case basis.
As CMS acknowledged, it has challenges keeping national Medicare coverage on pace with breakthrough-designated innovations. Some requests for NCDs have been on a list awaiting approval since 2014. Historically, CMS only processes about 6 NCDs per year. While there has been some acceleration in processing NCD approvals, CMS remains significantly behind the demand for and supply of innovative technologies.
CMS Coverage Changes and Challenges
The CMS proposed rule addresses the second criteria for Medicare coverage above, whether the item or service is medically reasonable and necessary. The proposed rule would supplant the previous coverage process which can take as long as 6 years and deem devices with breakthrough designation that are cleared by the FDA as medically reasonable and necessary as long as they are (1) safe and effective, (2) not experimental or investigational, and (3) appropriate for the Medicare patients. MCIT would be a revolutionary change in the CMS coverage process. But in its current form, the rule is largely toothless. As CMS notes in the rule, if there is no benefit category for the innovative technology, Medicare cannot cover or pay for it.
To date, CMS has not placed digital therapeutics into a benefit category. Existing efforts among the commercial payers and some Medicaid managed care organizations have successfully reimbursed digital therapeutics as DME, Telehealth, Pharmacy Benefit, Pharmacy Benefit as “Other related item” for a drug, incident to physician service, Remove Patient Monitoring, Value-add or In-lieu of Service in Medicaid, or a Supplemental Benefit for Medicare Advantage. (Ostrovsky et al 2020 in peer review)
However, in the absence of traditional Medicare coverage for SaMD, the reimbursement approaches in the commercial and Medicaid spaces require significant socializing and recreating the wheel of contractual arrangements each time a technology manufacturer seeks to establish a business relationship with a new payer. This redundancy adds to the wasteful spending in the already overly expensive American healthcare system and delays evidence-based treatments from getting to the patients.
Medicare has lagged behind the commercial space due to the lack of a digital therapeutic benefit category which has further widened the equity gap for American seniors, people with disabilities, people with ESRD, and other beneficiaries of traditional Medicare. To make matters worse, the COVID19 pandemic has disproportionately impacted Medicare beneficiaries, further exacerbating health disparities.
Digital therapeutics can meaningfully support virtual care and simultaneously facilitate social distancing while ensuring access to evidence-based interventions. While CMS has made meaningful strides during the COVID19 pandemic through its telehealth flexibilities, its outdated view on SaMD and digital therapeutics has limited CMS’s ability to close these health gaps.
In the early days of digital therapeutics, CMS was understandably reluctant to cover them. CMS’s reticence toward digital therapeutics stemmed from four root causes. First, the Medicare program’s staff have to thoroughly review the literature for new technologies and by their innovative nature, early digital therapeutics initially had limited research. Second, the Medicare program is obligated to avoid fraud, waste, and abuse to ensure good stewardship of taxpayer dollars. Third, CMS staff have residual fear from the Supreme Court hand-slap related to health technology whereby the high court ruled against some CMS rule-making procedural missteps in Allina v. Azar. Fourth, the CMS interpretation of the definition of DME is too concrete. These four drivers make CMS staff apprehensive to move out of their coding and coverage comfort zone.
The COVID19-induced public health demand for safe and effective socially-distanced interventions will persist for years and should push CMS out of its regulatory routine and habit. The four barriers to CMS’s coverage and reimbursement for digital therapeutics are not only outdated but also stifle equitable access to care for millions of Americans amid this pandemic. First, the rigor and quality of the digital therapeutic space has evolved dramatically over the last decade, largely to the credit of the FDA and its innovative and thoughtful approach to review SaMD leading to the creation of the BDP and culminating in the recent creation of the Digital Health Center of Excellence. The FDA’s evidence review as part of its clearance and approval process should suffice CMS’s need for proof of clinical efficacy. Second, the digital exhaust from digital therapeutics is much more granular and real-time than the analog paper trail for traditional DME when used for fraud, waste, and abuse detection and prevention. Additionally, the data supply from digital therapeutics could support improvement in outcomes or reductions in healthcare system costs. The value of these data could be incorporated into Medicare coverage and payment decisions. Third, with MCIT, CMS has appropriately followed rule-making protocol thus protecting CMS staff from getting burned by the legal hot water of Allina v. Azar. Fourth, based on the CMS DME coding decision tree and regulatory definition, many breakthrough-designated digital therapeutics meet criteria for creation of a new or miscellaneous HCPCS code as a DME benefit.
SaMD Could be Coded as DME
The importance of having an existing Medicare benefit category for the viability of MCIT warrants a thorough analysis of the treatment of breakthrough-designated digital therapeutic SaMD as DME. In response to the CMS HCPCS coding decision tree (Figure 3), SaMD applications or devices are capital equipment; most are not exclusively used in an inpatient setting; almost none are appropriate for a different code set given their breakthrough nature; and most would not qualify as a physician service. All breakthrough-designated SaMD are primarily medical in nature. Most of these technologies have mechanisms to lock access to the application or the device such that it can only be securely accessed by the patient for medically prescribed purposes. There will likely be several breakthrough-designated SaMDs that receive FDA clearance or approval in the coming years. Given the high prevalence, morbidity, and mortality among Medicare beneficiaries due to the chronic conditions that are treatable by breakthrough-designated digital therapeutics before COVID19 (especially and including behavioral health conditions), there has been a long-standing national program operating need for digital therapeutics. With COVID19 killing over 180,000 Medicare beneficiaries to date, the need for these innovative technologies that can safely deliver their therapeutic benefit in a socially-distanced setting has become much more pressing. By virtue of their breakthrough designation, most of the digital therapeutics will not have HCPCS codes that describe what they do. Finally, obtaining 3 months of market data is not a challenge for high quality breakthrough-designated technology companies.
Similar to the HCPCS coding decision tree, breakthrough-designated SaMD meet the DME regulatory definition according to 42 C.F.R. § 414.202. SaMD, and the smartphone or tablet on which it is being used, can withstand repeated use. Both SaMD can be designed to have an expected life of 3 years with the added benefit of software updates to ensure bugs are resolved and minor features are incorporated to improve the customer experience. As with the HCPCS decision tree, all breakthrough-designated SaMD are primarily and customarily used to serve a medical purpose. By the same token, these technologies would not be useful in the absence of an illness or injury by virtue of their ability to lock access to the application or the device such that it can only be securely accessed by the patient for medically prescribed purposes. By their mobile nature, SaMD are ideally suited for use in the home.
Conclusion
According to the CMS Administrator, reversing course on virtual care would be a mistake. The need for virtual care existed before COVID19 and will persist beyond it. This pandemic has served as a regulatory catalyst for advancing telehealth and with the introduction of the MCIT proposed rule, COVID19 can trigger advances in other virtual modalities to meet the needs of Medicare beneficiaries. But for the MCIT initiative to have teeth and fulfill its intent, CMS should clearly state that the DME benefit category applies to many digital therapeutics and clarify that breakthrough-designated SaMD could be subject to this coverage and subsequent payment. Doing so would help eliminate disparities in treatment for Medicare beneficiaries and balance accountable chronic disease management with the need for social distancing in the COVID19 era and beyond. To voice your perspective and improve equitable access to evidence-based digital therapeutics, please comment on the proposed rule here no later than November 2, 2020.