Centers for Medicare & Medicaid Services (CMS) recently published results detailing 2023 performance of the Medicare Shared Savings Program[1] (MSSP). The MSSP is a government-led program that encourages Accountable Care Organizations (ACOs) to reduce healthcare costs while improving quality of care for Medicare beneficiaries. This program incentivizes quality improvement and cost-containment by making these ACOs eligible to share in the medical-cost savings they achieve for the Medicare program, after they meet their quality goals. This program supports policies that CMS has adopted to enhance primary care, expand access for underserved communities, and prioritize quality care for chronic conditions.

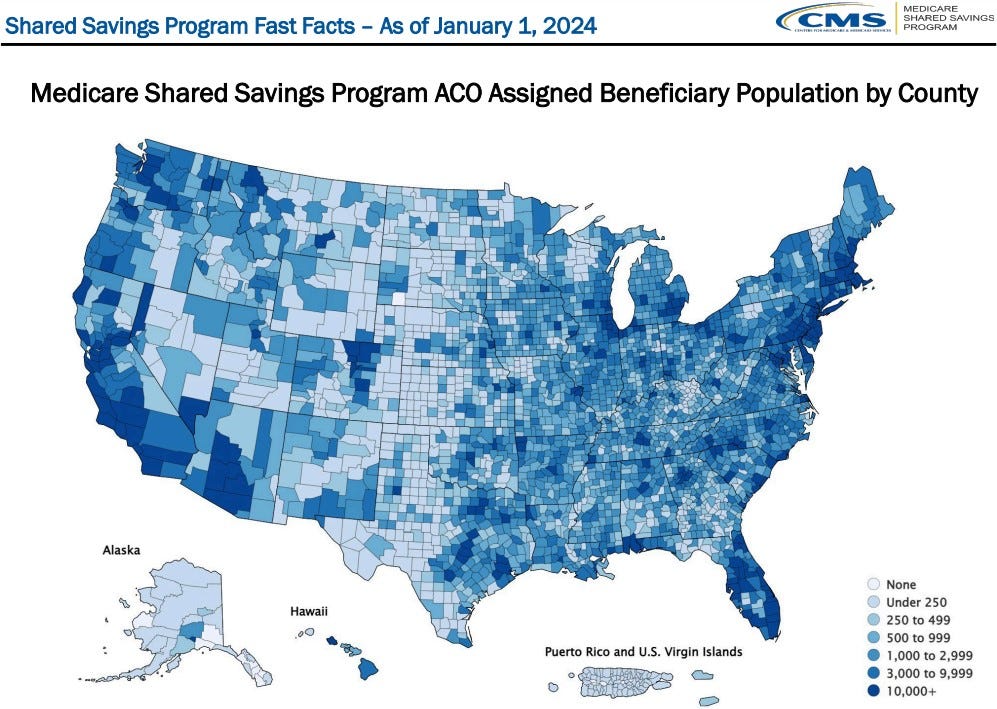
Figure 1: CMS 2024 Shared Savings Program Fast Facts. MSSP assigned beneficiary population by county (credit CMS.gov)
2023 MSSP Performance
This past year, the MSSP exhibited quality improvement among ACO providers and achieved its largest annual savings, reducing CMS’ medical expenditures on behalf of Medicare recipients by $5.2billion[1]. This constitutes a 4% per-capita reduction in spending for roughly 11million Medicare beneficiaries[2]. Of the overall savings achieved by ACOs, CMS retained $2.1billion of these savings. A total of 453 ACOs reconciled their performance against CMS benchmarks, and 69% of these ACOs achieved shared savings, earning a total of $3.1billion in performance payments. In addition to medical cost savings, ACO quality scores improved for the following categories[1]:
· diabetes and blood pressure control
· breast cancer and colorectal cancer screening
· screening for future fall risk
· statin therapy for prevention and treatment of cardiovascular disease
· depression screening and follow-up
Based upon the success of existing ACOs, CMS has set a goal that 100% of people with traditional Medicare will be part of an accountable care relationship by 2030[1].
What is an ACO?
Accountable Care Organizations (ACOs) are provider or hospital groups that collaborate to provide care for traditional Medicare enrollees. They have the joint goals of delivering high-quality care, and spending health care dollars (from CMS) efficiently, to provide that care. When an ACO meets or exceeds its care-quality targets, that ACO may be eligible to share in the medical cost savings that it generates for the Medicare program. ACOs may also share in losses if they increase spending. This provides a financial incentive for the providers who participate in ACOs to focus on efficiency and quality.
ACOs are incentivized (through quality metrics) to support CMS policies aimed at enhancing primary care, expanding access for underserved communities, and prioritizing quality care for chronic conditions[1].
Overall, ACOs have the effect of lowering healthcare costs for Medicare recipients by spending less money on avoidable care utilization (such as ER visits) by actively engaging patients in well-coordinated, preventative, and whole-person care.
How are ACO’s paid?
ACO providers are still paid by CMS on a Fee-For-Service (FFS) basis. Their ACO offices track quality measures and report them to CMS, and at the end of the performance period, provider payments are adjusted based upon the care quality performance of the overall ACO. Shared savings are calculated against a medical cost benchmark, which is a unique measure according to each ACOs contract. This benchmark may be past-year per-capita expenditures, a running average of prior performance, or comparisons to non-ACO FFS expenditures. The actual payments that an ACO receives and distributes to providers is determined using the “shared savings rate” which allocates a percentage of medical cost-savings to the ACO, and the remainder to CMS. Many ACO contracts institute caps protecting against extreme upside and downside risks, which have the effect of constraining the bonuses or losses an ACO may experience based upon their performance[3].
What conclusions can we draw from 2023 performance data?
The MSSP may be one of the first care models in US healthcare to effectively decrease medical expenditures while increasing the quality of care. The past 12 years of performance data show that properly aligning provider incentives can help accomplish the triple aim in healthcare: improving population health, reducing per-capita costs, and enhancing the patient experience.
2023 performance data also leads us to draw several logical conclusions:
1. Primary care is essential for early detection and management of health issues, which can prevent more serious and costly problems down the line. ACOs led by PCPs had significantly higher per-capita savings than ACOs with a smaller proportion of primary care doctors[1]. Primary care is also critical in capturing HCCs (Hierarchal Condition Categories) and accurately reflecting risk scores.
2. Risk Adjustment Factor (RAF) is still a crucial value-driver, despite the adoption of new coding standards (HCC V28) in 2024 that decreased RAFs across patient populations. ACOs with higher average RAF had a greater probability of achieving shared savings[1]. This indicates that properly capturing and coding HCCs is still important!
3. 78 of the 100 largest ACOs achieved shared savings, while only 64 of the 100 smallest ACOs achieved savings[1]. Larger ACOs have a greater probability of achieving shared savings than smaller ACOs, which can be attributed to their broad networks of primary care physicians and specialists that are aligned to the same quality and financial goals[1]. Preventing leakage, or ensuring that Medicare patients remain in an ACO’s network, allows an ACO greater control in pursuing quality metrics and keeping their patients out of acute care settings.
[1] https://www.cms.gov/newsroom/press-releases/medicare-shared-savings-program-continues-deliver-meaningful-savings-and-high-quality-health-care
[2] https://www.fiercehealthcare.com/payers/mssp-acos-saves-medicare-21-billion-2023-largest-savings-program-history
[3] https://www.mckinsey.com/industries/healthcare/our-insights/the-math-of-acos
About the author: Sam Jacobs is a Senior Product Manager on the Fusion team at UnitedHealth Group. Fusion accelerates key leaders and their teams by injecting a design thinking mindset and unleashing teams’ creative potential. Sam’s background is in biomedical engineering and medical device product management, which helps him to understand the challenges we face in today’s healthcare environment. Want to know more? You can find Sam on LinkedIn: https://www.linkedin.com/in/sam-jacobs-healthcare/
A Fusion publication. We are employees of UHG and these views are our own and not those of the company nor its affiliates.