OBBB Section (71112): Medicaid and CHIP Retroactive Coverage

So, what are the implications for healthcare providers and patients? As healthcare leaders navigate the evolving reimbursement landscape and policy reforms, it is essential to stay ahead of changes that could impact patient access, financial stability, and operational efficiency. One such shift is outlined in Section 71112 of the budget reconciliation measure passed in 2025. This provision, set to take effect in the first quarter following December 31, 2026, introduces limitations on retroactive coverage for Medicaid and the Children’s Health Insurance Program (CHIP).
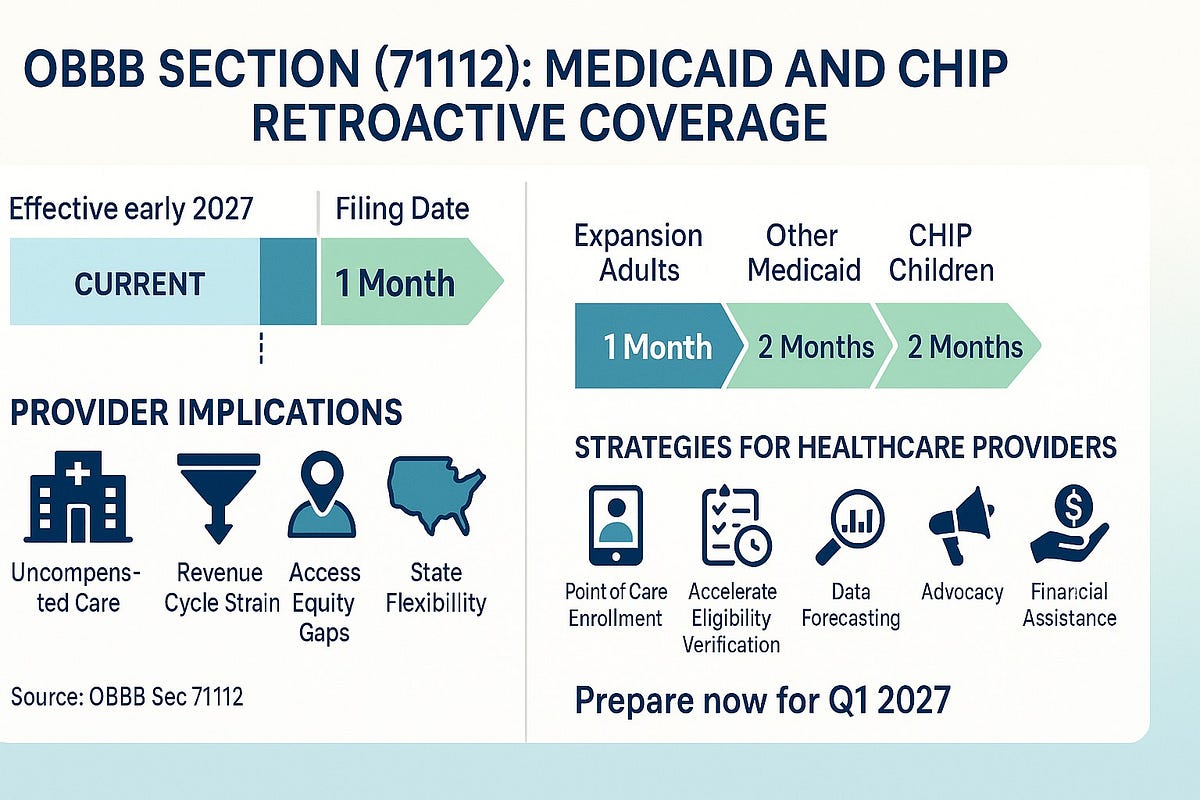
While aimed at controlling federal and state expenditures, these adjustments could have ripple effects on uncompensated care, revenue cycles, and equity in healthcare delivery. Understanding the Current Framework. Today, Medicaid and CHIP allow for retroactive coverage up to three months before the date an individual files their application. This longstanding policy has been a safety net, ensuring that eligible individuals — often facing sudden health crises — aren’t burdened with out-of-pocket costs for services received before formal enrollment. For hospitals, clinics, and other providers, this retroactivity has helped mitigate bad debt by reimbursing care that might otherwise go unpaid. There are key changes that you need to consider that will take effect in early 2027, and these rules will tighten your budget in several ways. First, is the Medicaid expansion population. The retroactive coverage will be limited to one month before the application filing date. This group, primarily adults aged 19–64 with incomes up to 138% of the federal poverty level in states that expanded Medicaid under the Affordable Care Act (ACA), will see the most significant reduction. Second, what will be the effects of this on all other Medicaid enrollees? For non-expansion groups, including children, pregnant individuals, seniors, and individuals with disabilities, retroactive coverage will be extended to two months before the application date. The third effect is on CHIP enrollees. CHIP coverage for children will provide retroactive coverage up to two months before the filing date.
These modifications represent a departure from the uniform three-month window, potentially aligning with broader fiscal goals in the OBBB to curb Medicaid spending growth. As a healthcare leader, you will need to consider an increase in uncompensated care. With shorter retroactive periods, more patients may face uncovered bills for services rendered two to three months before applying. This is particularly acute for the expansion population, where a one-month limit may leave gaps in coverage during emergencies, such as hospitalizations or surgeries. Providers may see a rise in charity care write-offs, straining already thin margins due to post-pandemic recoveries and inflation. In addition, there will be changes to the revenue cycle. Your billing teams will need to adapt processes to identify and pursue retroactive claims more swiftly. Expect heightened administrative burdens, including faster eligibility verifications and appeals. Organizations in states with high Medicaid penetration should audit current workflows to minimize denials. Another consideration is that access to care for vulnerable patient populations, including those in rural or underserved areas, may be delayed due to fears of unaffordable bills. This could exacerbate health disparities, especially in states that expanded Medicaid under the ACA, where the one-month cap applies to a larger share of enrollees. Leaders should advocate for enhanced outreach programs to encourage timely applications and explore partnerships with community organizations for enrollment support. Finally, while federal matching funds will enforce these limits, states retain flexibility in implementation. Some may seek waivers or invest in technology to streamline the application process, potentially softening the blow. Monitor your state’s Medicaid agency for guidance, as variations could affect local operations.
So, as a healthcare leader, what are some strategies that your team can use to mitigate risks? Consider these actionable steps. First, invest in digital tools and staff training to expedite Medicaid/CHIP applications at the point of care. Collaborations with navigators can reduce application lag times. Second, use data analytics to forecast the impact on your uncompensated care ratio. Simulate scenarios based on your payer mix to inform budgeting for 2027 and beyond. Stage engaged in advocacy and policy engagement at the state and federal levels. Join coalitions to push for mitigating measures, such as extended continuous eligibility periods already in place for children under recent CMS rules. Healthcare leaders need to engage with policymakers to highlight how these cuts might inadvertently increase long-term costs through worsened health outcomes. Lastly, but not least, develop financial assistance programs or implement sliding-scale fees to bridge coverage gaps, thereby fostering loyalty and community trust.