Here’s a piece I wrote about Medicaid in Pennsylvania for my Health Data class:
I. A brief history
Back in the early 80’s, Pennsylvania became one of the first states to bring the concept of Medicaid Managed Care to fruition. What started with a few Health Maintenance Organizations scattered throughout the state grew in 1986 with a waiver from the federal government to set up a Health Insuring Organization (HIO) through Pennsylvania’s Department of Public Welfare (DPW). Over the next 15 years, PA rolled our and trialed their HealthChoices (named HealthPASS until 1997) program, mandating that those under the 1986 waiver use the new Medicaid Managed Care system. And today, Medicaid recipients in Pennsylvania choose a Managed Care Organization (MCO), each of which guarantees access to a PCP and other services. These MCOs are paid a fixed amount by the DPW for each customer. This is now the model used across the country; more than 70% of US citizens on Medicaid receive their insurance through an MCO.
II. Pennsylvania and the Affordable Care Act
In September of 2014, Pennsylvania became the 27th state to expand Medicaid, after undergoing a review process of their plan by the federal government. Those eligible for Medicaid now have access to a low or high risk plan (before there were more than ten options), and are free from paying any deductibles until 2016. The implementation granted to PA, however, does not reflect the original plan put forward by soon-to-be-former Governor Corbett (R), which contained provisions such as payments up to $10 for non-emergency visits to an emergency room (the Federal plan reduced this down to $8), and deductibles for those above the poverty line up to 2% of income. Other denied requests include allowing more customizable benefits, the flexibility to deny non-emergency transportation benefits, and not having to pay for retroactive service.
As an aside, I believe Pennsylvania should expand the number of plans available to Medicaid recipients in order to better serve those on Medicaid and also reduce unnecessary costs. Since the Federal government denied PA the ability to provide more flexibility with regards to which benefits each plan provides, returning to multiple plans would allow people to receive covered care that they actually need, and forgo those they can do without.
Pennsylvania would also benefit from charging those at the high end of income for Medicaid eligible individuals a small premium to recoup some of the losses ensured by expansion. This would help reduce PA’s large deficit and would not be crippling to those who barely qualify for Medicaid.
The last implementation suggestion I would try to make would be to re-evaluate the places that funding is going — as we will see later in this report, PA is dreadful at providing quality nursing home care. If benefits were restructured such that Medicaid would pay more for nursing home care, that industry would receive more cash, which would almost assuredly, bring quality up.
III. Pennsylvania compared to the Nation
With the new expansion, Pennsylvania now falls in line with other nations expanding Medicaid in terms of eligibility. Pennsylvania also does a good job of insuring a high percentage of people who are eligible for Medicaid: 89% of those eligible compared to the national average of 88%. However, some PA falls behind in most other measure.
Data from a report titled “Unsettling Scores: A Ranking of State Medicaid Programs” shows that Pennsylvania ranks 33rd overall when taking into account eligibility, scope of services, quality of care, and reimbursement. PA does particularly bad in the reimbursement category: the amount doctors receive for treating Medicaid recipients is 79% of the value of the care given in PA. In the quality of care category, PA did particularly bad in quality of nursing homes and child immunization rate, but faired well in measures of staffing. The Scope of Services suffered due to lack of coverage of women’s services, rehabilitation, and equipment. PA did their relative best in eligibility, but still falls behind in insuring those with slightly more income than the poverty level.
The cost per person on Medicaid averaged $7,288 according to a 2010 report by the Kaiser Family Foundation, which is well above the average of $5563. This can largely be attributed to PA’s large population of senior citizens and their relatively higher cost of care.
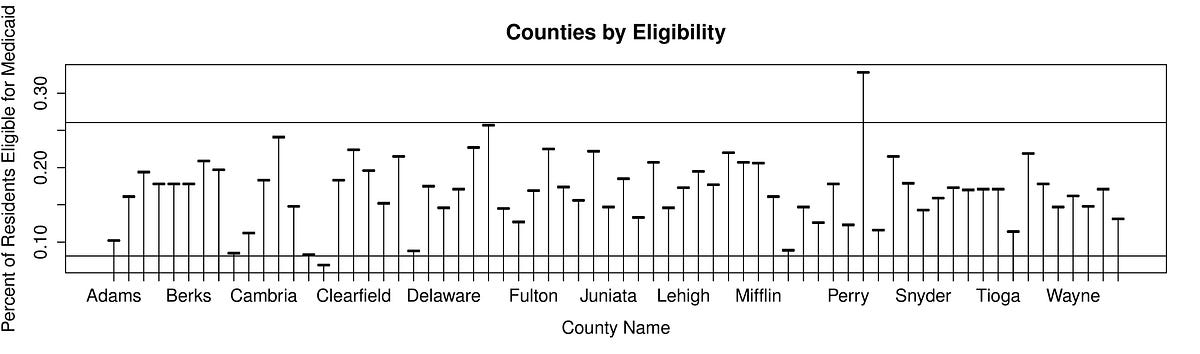
IV. An Analysis on County Data for Medicaid Eligibility

The question that I set out to answer with this dataset was: “How much disparity is there between counties in terms of percentage of people eligible for Medicaid?” This answer to this question will show the diversity of the needs of a state when it comes to Medicaid, and whether the state is largely homogenous in its need. The data I’m using comes from PA’s Department of Public Welfare’s April 2010 determination of the number of people eligible for Medicaid by County. I plotted the data by County in a line chart, and visually it is pretty easy to see how much variation exists between counties, with Philadelphia County by far having the highest percentage eligible. I added lines 2 standard deviations above and below the median to accentuate just how variable eligibility percentage is across county lines — many of the counties come close or exceed two standard deviations away from the median. This graphic made me believe that determining funding on a regional level while trying to standardize practices statewide must be very difficult when the needs of each county are so clearly different.